Simple Measures Can Improve Hand Hygiene for Quality Health Care
By Hassan Kasujja and John Paul Waswa, MTaPS Uganda
Health care associated infections (HAI) affect patients in Uganda at an average rate of 15%, per the 2019 National Infection Prevention and Control (IPC) report, going up to 34% in some health facilities. Hand hygiene has been recommended by the World Health Organization (WHO) as the most effective IPC intervention to reduce HAIs and as an entry point to implementing IPC programs, which are pivotal to safer, high-quality health care at health facilities. A key aspect of an effective hand hygiene program in a facility is monitoring the consumption of soap and alcohol-based hand rub (ABHR), which is indirectly indicative of success of the hand hygiene performance and which can also inform the purchasing frequency and amounts of the commodities needed for a continuous supply to sustain the hand hygiene program.
USAID MTaPS is implementing IPC and hand hygiene interventions in Uganda with the aim of improving these practices to reduce HAI rates and the spread of resistant bugs in facilities, in a bid to contain antimicrobial resistance (AMR) under its Global Health Security Agenda mandate. As a basis for informing hand hygiene interventions, in 2021, MTaPS applied the WHO soap and ABHR consumption tool—a first in Uganda—to assess hand hygiene practices at 13 health facilities: 6 public regional referral hospitals and 7 private-not-for-profit hospitals.

Building Hospital Capacity for Data Collection
The data collection process for tracking consumption of soap and ABHR began with an onsite one-day training of 3 health care workers from the IPC committee of each of the 13 facilities, facilitated by MTaPS technical staff. The health care workers learned about theoretical and practical mock application of the WHO soap and ABHR consumption tool. The trained team collected data on soap and ABHR consumption from the facilities’ stores for a period of 6 months and eventually analyzed the data with MTaPS’ support.
Assessment, Findings, and Insights
In an attempt to categorically link hand hygiene practiced at facilities to patient care, the average soap and ABHR consumption was computed in relation to the number of patient days (PD) at the respective facilities. Previous recordings of consumption of ABHR and soap did not relate it to patient days, falling too short to shed light on wastage or optimal utilization of these consumables.
Some findings:
- All facilities were found to use both ABHR, used mainly by health workers, and soap, mainly by patients and caregivers, with the average consumption by all facilities close to the ideal consumption of 40 ml/PD: 39.4mL/PD of ABHR and 39.9mL/PD of soap (figure 1).
- Private health facilities were found to consume more supplies than public health facilities—ABHR by 28% and soap by 11%—reflective of the more freely available commodities at private hospitals vis-à-vis the limited resources at public hospitals. The data by different facility types can also inform interventions based on the varying governance and supply chain mechanisms of private and public facilities.
Figure 1: Consumption of ABHR and soap in the assessed facilities
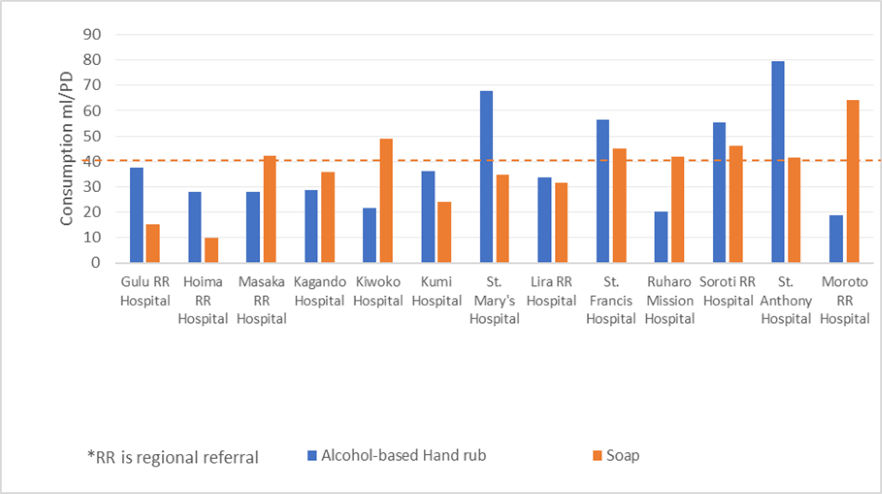
- The facilities’ average ABHR consumption was almost double the average consumption from a similar study conducted in 232 European hospitals in 2015 (reported average consumption: 21mL/PD). This could be due to interventions for mitigating the spread of COVID-19 in health facilities or misuse of ABHR in the assessed facilities. The high ABHR use was found not to be linked to patient care, as it is used by staff even when at home and by students and support staff at the facilities, evidenced by the example of St. Anthony’s Hospital, which had the lowest number of patients, yet the highest consumption per patient day.
- Most of the soap consumed was found to be for use by caretakers and visitors, which is also key in protecting patients from health threats from the caretakers and must be monitored and supplied adequately for patient safety.
Conclusion: Data-Driven Recommendations and Future Interventions
- With the high consumption found in facilities, the hospitals would benefit from an expanded program of local manufacture of ABHR, cutting the cost from about 2.61 USD to 0.47 USD per 100 ml ABHR as per the WHO guidelines for local manufacture of ABHR.
- Both underuse and overuse, which can cause stockout, can undermine patient care and are risk factors for increased HAI rates in facilities. The simple intervention of routine data collection of commodities can help address supply chain gaps and indirectly monitor hand hygiene performance. Therefore, consumption of ABHR and soap is recommended to be added as an indicator in the annual national IPC assessment.
- In the aftermath of COVID-19 and based on MTaPS’ assessment, the Ugandan Ministry of Health is developing a strategy to ensure use and availability of ABHR through strengthening local manufacturing capabilities at the facility level, which will be included in the National IPC Strategic Plan under development.
- Facilities and countries should invest in monitoring and costing ABHR and soap consumption—a relatively low-cost investment with low skill requirements that will contribute to optimal use of these commodities and avoiding their stockout—a key aspect of reducing HAIs for quality health care and containing AMR for greater global health security.